Executive Summary
In the intricate ecosystem of healthcare Revenue Cycle Management (RCM), the ICD-10-CM (International Classification of Diseases, 10th Revision, Clinical Modification) code set serves as the absolute foundation of reimbursement. While CPT codes tell the insurance payer what service was provided, ICD-10 codes tell the payer why it was provided. If the "why" is not communicated with surgical precision, the payer’s automated adjudication engine will instantly reject the claim for lack of medical necessity (CARC CO-11). Despite this, countless independent practices continue to bleed revenue due to truncated diagnosis codes, a reliance on outdated "unspecified" defaults, and a fundamental disconnect between the physician's clinical documentation and the coder's requirements. This comprehensive guide dissects the crippling financial impact of ICD-10 coding errors, explores the rigid mechanics of Local Coverage Determinations (LCDs), and provides practice leaders with a robust framework for Clinical Documentation Improvement (CDI) to guarantee first-pass claim payment.
Key Takeaways
- Specificity equals Revenue: Submitting "unspecified" ICD-10 codes (often ending in .9) is the fastest way to trigger a manual payer review or a flat-out denial for high-cost procedures.
- The LCD/NCD Barrier: Medicare and commercial payers maintain strict lists (Local and National Coverage Determinations) detailing exactly which ICD-10 codes justify which CPT codes. Deviating from this list guarantees a denial.
- Laterality and Episode of Care: ICD-10 requires granular details that ICD-9 never did, including exact anatomical laterality (left, right, bilateral) and the specific episode of care (initial, subsequent, sequela).
- The CDI Imperative: Certified coders cannot invent specificity; they can only code what the physician writes. Clinical Documentation Improvement (CDI) training for providers is mandatory for revenue preservation.
- Annual Updates are Critical: The ICD-10 code set updates every October 1st. Failure to update practice management software and superbills on this exact date results in catastrophic, practice-wide denials.
Table of Contents
- The Anatomy of an ICD-10 Code
- ICD-10 and the Burden of Medical Necessity (CO-11)
- The Top 4 Most Damaging ICD-10 Coding Errors
- The Compound Financial Impact of Diagnosis Errors
- Clinical Documentation Improvement (CDI): The Ultimate Solution
- Case Study: Rescuing a New York Pain Management Clinic
- Action Plan: Eradicating ICD-10 Denials in Your Practice
- Why Independent Practices Rely on Outsourced AAPC Coders
- Conclusion
1. The Anatomy of an ICD-10 Code
To understand how an ICD-10 error destroys revenue, one must first understand the structural mechanics of the code set itself. The United States transitioned from ICD-9 (which had roughly 14,000 codes) to ICD-10 (which contains over 70,000 codes) to allow for unprecedented clinical granularity.
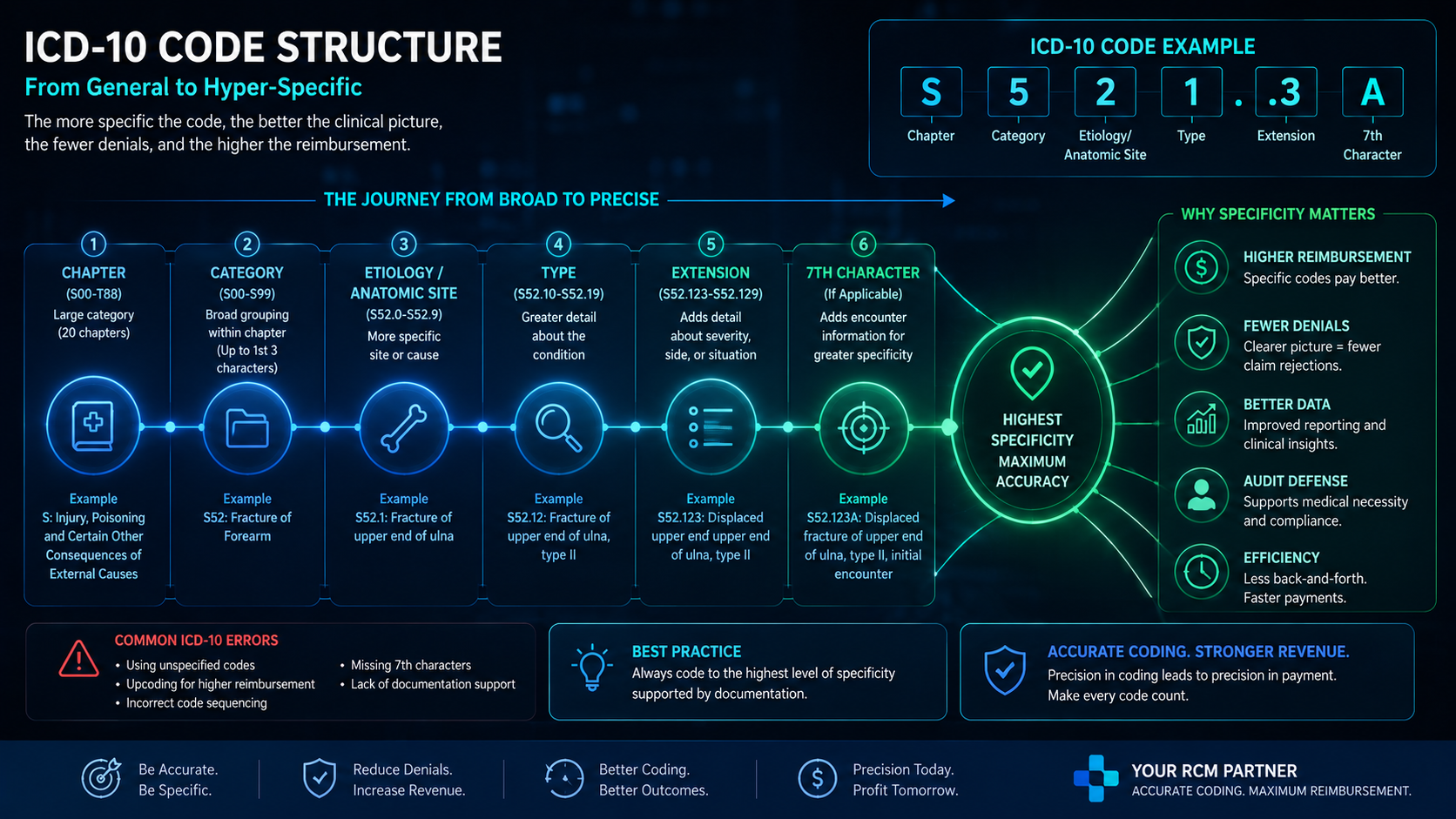
An ICD-10-CM code contains between 3 and 7 characters:
- Characters 1-3: Category of the disease or condition (e.g., S82 - Fracture of lower leg).
- Characters 4-6: Etiology, anatomic site, severity, or other vital clinical details (e.g., S82.021 - Displaced fracture of patella, right knee).
- Character 7: Extension representing the episode of care (e.g., S82.021A - Initial encounter for closed fracture).
If a coder submits a 4-character code when a 7-character code is clinically available and required by the tabular list, the claim is considered "truncated." The clearinghouse or the payer will immediately reject the claim as invalid.
2. ICD-10 and the Burden of Medical Necessity (CO-11)
The most devastating consequence of poor ICD-10 coding is the Medical Necessity Denial, represented on an Electronic Remittance Advice (ERA) by CARC CO-11: The diagnosis is inconsistent with the procedure.
Insurance payers do not pay for procedures simply because a physician ordered them; they pay for procedures that are proven to be medically necessary to treat a specific, highly detailed diagnosis. They enforce this rule via Local Coverage Determinations (LCDs) and National Coverage Determinations (NCDs).
3. The Top 4 Most Damaging ICD-10 Coding Errors
When revenue cycle audits are performed on struggling practices, the same four ICD-10 errors appear with alarming frequency:
Error 1: The Overreliance on "Unspecified" Codes
Because EMR drop-down menus are often cumbersome, physicians frequently select the first generic code they see (e.g., "Asthma, unspecified"). While unspecified codes were heavily tolerated during the initial years of the ICD-10 rollout, commercial payers and Medicare have aggressively cracked down. Today, an unspecified code attached to a high-cost procedure is almost a guaranteed denial.
Error 2: Missing Laterality
The human body is bilateral. ICD-10 requires the coder to specify left, right, or bilateral. If a provider injects a patient's left shoulder but the clinical note just says "shoulder injection," the coder cannot legally guess. They must query the provider, delaying the claim, or submit an unspecified code, ensuring a denial.
Error 3: Ignoring Excludes1 and Excludes2 Notes
The ICD-10 tabular list contains strict instructional notes. An Excludes1 note indicates a "pure excludes"—meaning the two conditions cannot possibly exist together (e.g., a congenital condition cannot be billed alongside an acquired version of the same condition). Billing two codes that violate an Excludes1 edit triggers an immediate automated denial.
Error 4: Incorrect Use of the 7th Character Extension
In injury and fracture care (Chapter 19), the 7th character is mandatory to denote the phase of treatment: 'A' for initial encounter, 'D' for subsequent encounter, or 'S' for sequela (late effect). Submitting an 'A' for a patient returning to have a cast removed will result in a denial, as the payer's system recognizes the patient has already had their initial surgical encounter.
4. The Compound Financial Impact of Diagnosis Errors
Many practice owners view coding errors as mere administrative nuisances. In reality, they are severe financial hemorrhages.
- The Cost of Rework: The Medical Group Management Association (MGMA) estimates that it costs approximately $25 in administrative labor to rework a single denied claim. If your practice suffers 300 medical necessity denials a month due to poor ICD-10 specificity, you are losing $7,500 a month in pure administrative waste.
- Aging A/R Bloat: Claims denied for CO-11 require the coder to reopen the chart, query the physician, amend the clinical note, and submit an appeal. This process routinely takes weeks, pushing the claim into the dangerous >90 Day Accounts Receivable bucket where collection probability plummets.
- Audit Triggers: Payers track "aberrant coding patterns." If a provider's data profile shows a disproportionate use of unspecified codes compared to their peers, the payer will initiate a pre-payment audit, freezing all incoming revenue until the practice proves compliance.
5. Clinical Documentation Improvement (CDI): The Ultimate Solution
The golden rule of medical coding is simple: If it wasn't documented, it wasn't done. A certified coder is not a mind reader; they are a translator. If the clinical note lacks specificity, the resulting ICD-10 code will lack specificity.
To break this destructive cycle, elite healthcare organizations implement Clinical Documentation Improvement (CDI) programs. CDI is a collaborative process where AAPC-certified coders train clinical staff on exactly what details must be captured in the EMR during the patient encounter.
Poor Documentation (Guaranteed Denial)
"Patient presents with severe back pain and leg pain. Ordered MRI. Sent home with prescriptions."
Coder outcome: Forced to use M54.9 (Unspecified back pain). MRI claim denied.
CDI-Optimized Documentation (Guaranteed Payment)
"Patient presents with chronic left-sided sciatica secondary to L4-L5 lumbar disc herniation. Ordered MRI of lumbar spine without contrast."
Coder outcome: Uses M54.32 (Sciatica, left side) & M51.26 (Other intervertebral disc displacement, lumbar). MRI claim paid.
6. Case Study: Rescuing a New York Pain Management Clinic
The Medical Necessity Crisis
The Client: An interventional pain management clinic in New York. The physicians were performing high-value procedures, including epidural steroid injections (ESIs) and radiofrequency ablations, but their first-pass clean claim rate had plummeted to 72%.
The Diagnosis: An RCM audit by Axon Claim revealed that 80% of their denials were CO-11 (Diagnosis inconsistent with procedure). The physicians were relying on quick "macro" text blocks in their EMR that populated generic ICD-10 codes (like M54.5 - Low back pain). Medicare and commercial payers had recently updated their LCDs, explicitly stating that generic back pain no longer justified an epidural injection.
The Axon Claim Intervention:
- We initiated an aggressive CDI protocol. Our certified coders trained the physicians to document the exact neurogenic claudication, radiculopathy, and spinal stenosis details required by the new LCD guidelines.
- We rebuilt their EMR templates with "hard stops" requiring the physician to select laterality (left/right/bilateral) before locking the chart.
- The Results: Within 45 days, the clinic’s clean claim rate surged to 97%. Medical necessity denials essentially vanished, accelerating cash flow and allowing the practice to recover $180,000 in previously stalled claims.
7. Action Plan: Eradicating ICD-10 Denials in Your Practice
To eliminate the financial drain of diagnosis-driven claim denials, practice owners and billing managers should execute the following operational steps immediately:
- Run a Frequency Report: Pull an ICD-10 frequency report from your EMR. Identify your top 20 most utilized diagnosis codes. If any of those top 20 codes contain the word "unspecified," you have found your primary revenue leak.
- Audit the LCDs: Have your lead coder review the Local Coverage Determinations (LCDs) for your practice's top 10 most expensive CPT procedures. Create a cheat sheet for the providers showing exactly which specific ICD-10 codes currently justify those procedures.
- Prepare for October 1st: The CDC updates the ICD-10 code set annually on October 1st (adding, deleting, and modifying thousands of codes). Ensure your EMR and clearinghouse are systematically updated at midnight on September 30th to prevent mass rejections.
- Implement Pre-Bill Scrubbing: Utilize advanced RCM clearinghouse software that cross-checks the selected ICD-10 code against the CPT code and the payer's specific rules before the claim leaves the building.
8. Why Independent Practices Rely on Outsourced AAPC Coders
Expecting an overwhelmed front-desk receptionist or an uncertified "biller" to master the annual updates, Excludes1 notes, and LCD requirements of the ICD-10 manual is an operational impossibility. It places the financial health of the practice in the hands of untrained personnel.
For high-performing independent practices across New York, New Jersey, and nationwide, the solution is strategic outsourcing. Partnering with a premium Revenue Cycle Management firm like Axon Claim provides immediate, uninterrupted access to AAPC-certified coding experts. These specialists do not just punch data; they actively audit charts, query physicians for CDI, and ensure that every claim meets the absolute highest standard of medical necessity before submission.
9. Conclusion
The transition from ICD-9 to ICD-10 permanently altered the landscape of medical billing. Insurance payers now possess the algorithmic capability to demand absolute clinical precision before releasing funds. In this environment, "good enough" documentation results in devastating revenue losses.
By eradicating unspecified codes, mastering LCD requirements, and fostering a collaborative Clinical Documentation Improvement (CDI) culture between physicians and certified coders, medical practices can fortify their revenue cycle. Accurate ICD-10 coding is no longer just an administrative duty—it is the shield that protects your cash flow from the aggressive denial tactics of modern insurance payers.
Axon Claim LLC – Certified Coding Experts
We are a premier Revenue Cycle Management partner dedicated to helping healthcare providers across NY, NJ, and the US maximize their revenue. From advanced ICD-10 specificity to aggressive denial management, we protect your practice's financial health.
Are "Unspecified" Codes Killing Your Revenue?
A single generic code can trigger a wave of medical necessity denials. Let our AAPC-certified experts audit your top 20 ICD-10 codes for free to find your hidden revenue leaks.
Request a Free Coding AuditStop Leaving Money on the Table