Executive Summary
At the core of the healthcare Revenue Cycle Management (RCM) engine lies medical coding—a highly specialized discipline that translates complex clinical narratives into alphanumeric data (ICD-10, CPT, and HCPCS) used by insurance payers for reimbursement. While many practices treat coding as a simple administrative data-entry task, it is, in reality, the highest-risk focal point for both financial leakage and legal liability. Inaccurate coding manifests in two equally destructive ways: undercoding, which hemorrhages legally earned revenue, and overcoding (upcoding), which invites devastating federal compliance audits and financial penalties from the Office of Inspector General (OIG). This comprehensive guide explores the operational imperative of utilizing AAPC-certified coders, dissects the dangers of EMR auto-coding, and provides practice owners with a strategic framework to ensure clinical documentation perfectly aligns with stringent payer guidelines to maximize cash flow and eliminate compliance risks.
Key Takeaways
- The Dangers of Auto-Coding: Relying exclusively on EMR "suggested codes" without human certified review frequently leads to unbundling errors, modifier mismatches, and automated payer denials.
- Upcoding vs. Downcoding: Upcoding is a federal compliance violation (fraud), while downcoding—often done out of fear of an audit—is a guaranteed way to permanently sacrifice 15% to 20% of a practice's gross revenue.
- Medical Necessity is Paramount: A perfectly applied CPT code will still be denied if the corresponding ICD-10 diagnosis code does not meet the payer’s Local Coverage Determination (LCD) for medical necessity.
- Modifier Mastery: The incorrect use of modifiers (especially Modifiers 25, 59, and 76) is the leading trigger for RAC (Recovery Audit Contractor) audits.
- Outsourcing to Specialists: High-performing independent practices increasingly outsource their coding to specialized RCM firms to guarantee AAPC-certified precision and insulate themselves from liability.
Table of Contents
- What is Medical Coding in the RCM Ecosystem?
- The Dual Financial Impact: Undercoding vs. Upcoding
- Understanding Compliance Audits (RAC, OIG, and Payer Audits)
- The Top 5 Most Expensive Medical Coding Errors
- The Crucial Role of Clinical Documentation Improvement (CDI)
- Case Study: Rescuing a New Jersey Orthopedic Group from a RAC Audit
- A Step-by-Step Framework for Achieving 98% Coding Accuracy
- Why Elite Practices Outsource to Certified Coders
- Conclusion
1. What is Medical Coding in the RCM Ecosystem?
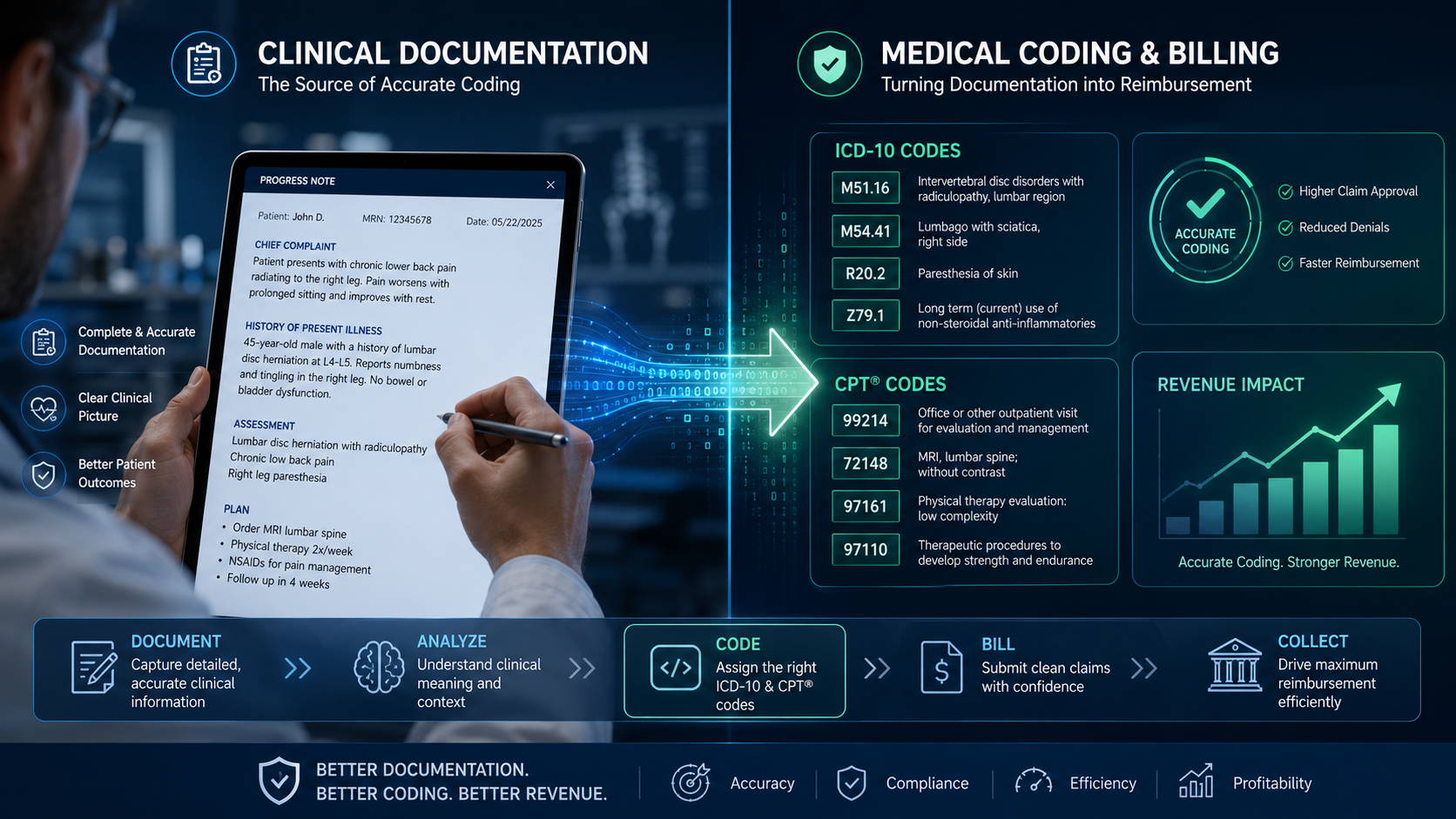
When a physician examines a patient, performs a surgery, or orders a lab test, the clinical details of that encounter are documented in the Electronic Medical Record (EMR). However, insurance companies do not read lengthy clinical paragraphs to determine reimbursement; they read data.
Medical coding is the highly specialized process of translating that complex clinical narrative into a universal alphanumeric language. This language consists of three primary code sets:
- ICD-10-CM (International Classification of Diseases, 10th Revision): These codes describe the patient's diagnosis or symptom (the "Why" the patient is being seen). They are incredibly granular—distinguishing not just a fractured arm, but specifically a displaced fracture of the distal phalanx of the left index finger.
- CPT (Current Procedural Terminology): Maintained by the AMA, these codes describe the specific medical, surgical, or diagnostic procedures performed (the "What" was done to the patient).
- HCPCS Level II: These codes represent products, supplies, and services not included in the CPT system, such as durable medical equipment (DME), prosthetics, and specific injectable drugs.
If the ICD-10 diagnosis code does not clinically justify the CPT procedure code according to strict payer guidelines, the claim is instantly denied for "lack of medical necessity."
2. The Dual Financial Impact: Undercoding vs. Upcoding
In medical coding, accuracy must be absolute. Missing the mark in either direction carries severe consequences.
The Danger of Upcoding (Overcoding)
Upcoding occurs when a provider or biller submits a code for a more expensive service or procedure than the one actually performed. A common example is consistently billing a Level 4 Evaluation and Management (E/M) visit (CPT 99214) when the clinical documentation only supports a brief, low-complexity Level 2 visit (CPT 99212).
Upcoding is not just a billing error; under the False Claims Act, it is considered healthcare fraud. Whether intentional or accidental due to poor training, upcoding triggers severe financial penalties, federal audits, and in extreme cases, the revocation of a provider’s medical license.
The Tragedy of Downcoding (Undercoding)
Conversely, many physicians, terrified of triggering a federal audit, intentionally "downcode" their services. They perform a highly complex, 45-minute Level 5 consultation but only bill a Level 3 code to "stay under the radar."
While downcoding may keep the auditors away, it is financial suicide. A practice that consistently downcodes its E/M visits is voluntarily forfeiting 15% to 25% of its gross revenue. Certified medical coders ensure that providers capture every dollar they have legally and ethically earned based strictly on what is documented in the chart.
3. Understanding Compliance Audits (RAC, OIG, and Payer Audits)
The healthcare industry is one of the most heavily audited sectors in the United States. Payers use sophisticated data-mining algorithms to detect statistical anomalies in a provider's coding patterns compared to their peers.
- RAC Audits: Recovery Audit Contractors (RACs) are independent companies hired by Medicare to identify and recover improper payments. Because RACs are paid on a contingency fee basis (they keep a percentage of what they claw back), they are hyper-aggressive in their scrutiny of E/M levels and modifier usage.
- Commercial Payer Audits: Private insurers like UnitedHealthcare and Aetna routinely flag practices that overuse certain high-value CPT codes or unbundle procedures. They will issue widespread records requests, suspending payments until the practice proves medical necessity.
The only defense against an audit is immaculate, defensible coding backed by pristine clinical documentation.
4. The Top 5 Most Expensive Medical Coding Errors
A lack of dedicated, certified coding expertise invariably leads to the following revenue-destroying errors:
1. Unbundling Services
The National Correct Coding Initiative (NCCI) dictates that many minor procedures are included in the payment for a major procedure. Billing these components separately is known as unbundling. The payer will instantly deny the secondary codes, delaying the entire claim.
2. Modifier Misuse
Modifiers alter the meaning of a CPT code. Improperly applying Modifier 25 (Significant, separately identifiable E/M service on the same day as a procedure) or Modifier 59 (Distinct procedural service) is the fastest way to trigger a payer audit.
3. Truncated Diagnosis Codes
ICD-10 codes require high specificity, often requiring up to 7 characters. Submitting a truncated, non-specific code (e.g., billing "unspecified asthma" instead of "mild intermittent asthma, uncomplicated") will result in an immediate medical necessity denial.
4. Reliance on "Cheat Sheets"
Many practices still use outdated, laminated "cheat sheets" or superbills. CPT and ICD-10 guidelines change annually on October 1st and January 1st. Using last year's codes guarantees sweeping denials across the practice.
5. The Crucial Role of Clinical Documentation Improvement (CDI)
A certified medical coder is highly skilled, but they are legally forbidden from guessing. They can only code exactly what the physician has explicitly written in the clinical note. If the documentation is vague, the coding will be vague, and the claim will be denied.
This is why elite RCM strategies incorporate Clinical Documentation Improvement (CDI). CDI involves coders working directly with physicians to improve the specificity of their charting.
6. Case Study: Rescuing a New Jersey Orthopedic Group from a RAC Audit
The Compliance Nightmare
The Client: A rapidly growing orthopedic and sports medicine practice in New Jersey. They relied entirely on the "auto-suggested" codes generated by their EMR system and utilized uncertified front-desk staff to submit the claims.
The Crisis: The practice received a devastating letter from a Medicare Recovery Audit Contractor (RAC). The RAC had flagged the practice for a 94% utilization rate of Modifier 25 alongside joint injections, demanding a massive clawback of over $250,000 for "improper unbundling."
The Axon Claim Intervention: The practice immediately engaged Axon Claim’s certified coding experts.
- The Audit Defense: Our AAPC-certified coders systematically reviewed the flagged charts. We discovered the physicians were, in fact, performing complex, separate E/M exams, but their EMR templates were not properly capturing the distinct documentation required to support Modifier 25.
- Workflow Correction: We successfully appealed the majority of the clawbacks by manually extracting the clinical evidence. We then completely overhauled their EMR templates to force strict CDI compliance for future visits.
- The Result: The practice was saved from a catastrophic financial penalty. Axon Claim subsequently took over their entire coding department, ensuring 100% compliance with NCCI edits and dropping their denial rate to below 3%.
7. A Step-by-Step Framework for Achieving 98% Coding Accuracy
To insulate your practice from federal audits and simultaneously maximize cash flow, implement the following operational framework immediately:
- Hire Only Certified Professionals: Never allow uncredentialed staff to assign or modify CPT/ICD-10 codes. Utilize only AAPC or AHIMA certified coders who possess specialty-specific experience.
- Conduct Quarterly Internal Audits: Do not wait for the government to audit you. Have an independent third party randomly audit 10 to 20 charts per provider every quarter to identify systemic upcoding or downcoding trends.
- Disable EMR "Auto-Coding": Relying on an EMR algorithm to generate a final bill is a massive compliance risk. Algorithms do not understand the nuanced clinical intent required to bypass NCCI edits. All auto-generated codes must be reviewed by a human expert.
- Invest in Physician CDI Training: Schedule bi-annual workshops where your certified coders train the clinical staff on exactly how to document to the highest level of specificity required by modern ICD-10 guidelines.
8. Why Elite Practices Outsource to Certified Coders
Maintaining an internal team of highly trained, AAPC-certified medical coders is incredibly expensive and difficult, particularly given the nationwide shortage of credentialed health information professionals.
For independent practices, multi-specialty clinics, and surgical centers across New York and New Jersey, outsourcing the coding and billing function to a specialized RCM firm is a strategic necessity. A premium partner like Axon Claim provides immediate access to specialty-specific certified coders who guarantee compliance, eliminate unbundling denials, and ensure that every legally earned dollar is captured and collected.
9. Conclusion
Accurate medical coding is not a back-office afterthought; it is the fundamental language of healthcare revenue. When a practice fails to respect the complexity of ICD-10, CPT, and NCCI guidelines, it exposes itself to catastrophic federal audits and silently hemorrhages cash through unworked denials and fearful downcoding.
By prioritizing Clinical Documentation Improvement (CDI), enforcing rigorous internal audits, and relying exclusively on AAPC-certified experts, healthcare organizations can achieve a state of bulletproof compliance. Master your medical coding, and you will fundamentally secure the financial prosperity of your practice.
Axon Claim LLC – Certified Medical Coders
We are a premier Revenue Cycle Management partner dedicated to helping healthcare providers across NY, NJ, and the US maximize their revenue. From AAPC-certified medical coding to aggressive denial management, we protect your practice's financial health.
Are You Afraid of an Audit?
Downcoding out of fear is costing your practice thousands. Let our AAPC-certified coding experts conduct a free, confidential chart audit to uncover your hidden compliance risks and revenue leaks.
Request a Free Coding Audit100% Secure & Confidential

