Executive Summary
Medical billing is not a monolithic discipline. While primary care billing revolves around predictable Evaluation and Management (E/M) codes, specialty billing—encompassing disciplines like Orthopedics, Cardiology, Gastroenterology, and Pain Management—is an entirely different operational beast. Specialty practices execute high-complexity, high-dollar surgical procedures that are ruthlessly scrutinized by insurance payer adjudication engines. A single misunderstanding of the Global Surgical Period, or a failure to append a distinct procedural Modifier (like 59 or 25), will trigger automated National Correct Coding Initiative (NCCI) unbundling denials, costing the practice thousands of dollars instantly. This comprehensive guide dissects the unique coding challenges inherent to specialty practices, providing surgeons and clinical administrators with the precise modifier strategies and Clinical Documentation Improvement (CDI) workflows required to safely maximize reimbursement and survive targeted federal audits.
Key Takeaways
- The NCCI Minefield: Medicare's National Correct Coding Initiative strictly prohibits billing multiple CPT codes together if one is considered a component of the other. Mastering NCCI edits is mandatory for surgical practices.
- Modifier 59 is a Target: Known as the "Distinct Procedural Service" modifier, Modifier 59 bypasses NCCI edits. Because it is highly abused, the OIG heavily audits its usage. Documentation must explicitly prove a separate anatomic site or separate encounter.
- The Global Surgical Period: Major surgeries include 90 days of post-operative care in the initial fee. Billing an E/M visit for a routine wound check during this period without the correct modifier (like 24) constitutes fraud.
- Modifier 25 Mastery: If a specialist evaluates a patient and performs a minor procedure on the exact same day, Modifier 25 must be appended to the E/M code to prove the evaluation was "significant and separately identifiable."
- Specialty Certification is Required: A general family practice coder cannot code a complex multi-vessel cardiac catheterization. Specialty practices must employ coders with discipline-specific AAPC certifications (e.g., CASCC, CCC, CGIC).
Table of Contents
- Why Specialty Billing is Fundamentally Different
- Understanding NCCI Edits and Unbundling
- Mastering the High-Risk Surgical Modifiers (25, 59, 24)
- Navigating the Global Surgical Period
- Deep Dive: Orthopedic & Pain Management Billing
- Deep Dive: Cardiology & Gastroenterology Billing
- Case Study: Rescuing an Orthopedic Group’s Spine Revenue
- Why Specialty Practices Must Outsource to Certified Experts
- Conclusion
1. Why Specialty Billing is Fundamentally Different
In a primary care setting, the revenue cycle is driven by volume. A physician sees 30 patients a day, billing relatively low-dollar Level 3 or Level 4 Evaluation and Management (E/M) codes. Denials, while annoying, are usually small.
In a specialty setting, the revenue cycle is driven by high-dollar procedural complexity. A spinal fusion or a complex cardiac ablation can generate thousands of dollars in a single claim. Consequently, insurance payers deploy advanced algorithms to aggressively scrutinize these claims.
Specialty billing requires a coder to read a complex, multi-page Operative Report and extract the precise anatomical locations, the specific surgical approaches used, and the exact devices implanted. A missed detail—such as failing to note that a procedure was performed bilaterally—can result in the practice losing 50% of the rightful reimbursement.
2. Understanding NCCI Edits and Unbundling
The single greatest threat to specialty revenue is the National Correct Coding Initiative (NCCI). Developed by Medicare (and adopted by all commercial payers), NCCI edits prevent practices from "unbundling" services.
Unbundling occurs when a practice bills multiple individual CPT codes for the separate components of a surgery, instead of utilizing the single, comprehensive CPT code that covers the entire procedure.
3. Mastering the High-Risk Surgical Modifiers (25, 59, 24)
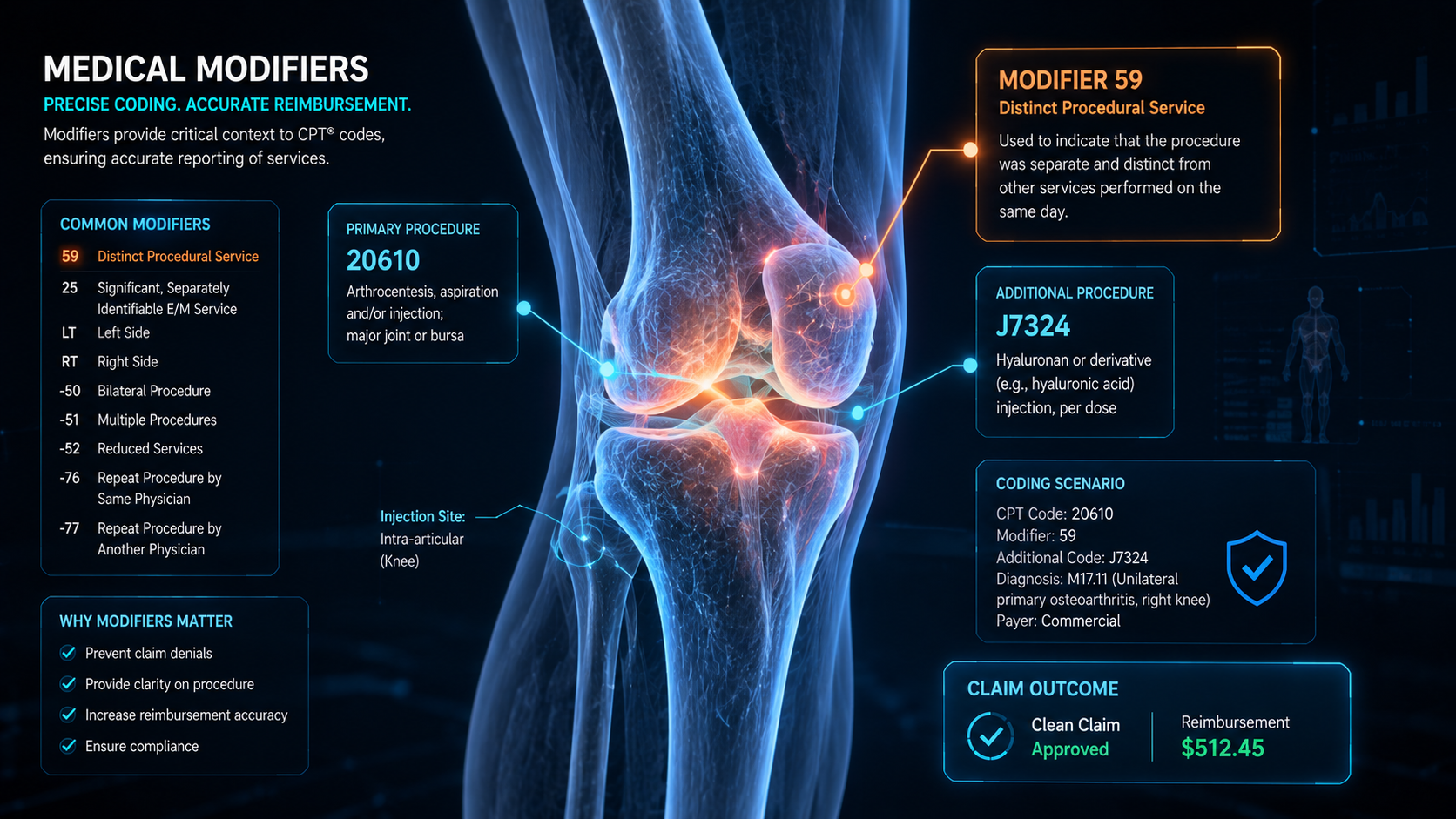
Modifiers are two-digit alphanumeric codes appended to a CPT code. They tell the insurance payer that a service was altered by a specific circumstance, but the definition of the code has not changed. In specialty billing, modifiers are the keys that unlock bundled NCCI edits—which is exactly why the federal government audits them so aggressively.
Modifier 59: Distinct Procedural Service
Modifier 59 is the most audited modifier in medical billing. It is used to bypass an NCCI edit by stating: "Yes, I know these two codes are normally bundled, but in this specific instance, they were performed on different anatomical sites, through separate incisions, or during separate patient encounters on the same day."
Risk: Overusing Modifier 59 without explicit documentation of a "separate and distinct" site will trigger a devastating Recovery Audit Contractor (RAC) audit.
Modifier 25: Significant, Separately Identifiable E/M Service
If a dermatologist evaluates a patient for a suspicious mole (E/M visit) and then decides to biopsy that mole (Procedure) on the exact same day, they must append Modifier 25 to the E/M code. This tells the payer that the evaluation went above and beyond the standard pre-operative care required for the biopsy.
Modifier 24: Unrelated E/M by the Same Physician During a Postoperative Period
If an orthopedic surgeon is in the 90-day global period for a patient's right knee replacement, and the patient comes in because they broke their left wrist, the surgeon must append Modifier 24 to the wrist visit. Without it, the payer will assume the visit is a free post-op check for the knee and deny the claim.
4. Navigating the Global Surgical Period
Medicare assigns a "Global Period" to almost every surgical procedure: 0 days, 10 days (minor procedures), or 90 days (major surgeries).
The fee the insurance company pays for the surgery includes the pre-operative visit (usually the day before), the surgery itself, and all routine post-operative care within the global period. You cannot bill an E/M code for routine post-op care during this window.
The Operational Challenge: The front desk and the billing team must have a tracking system to know exactly when a patient is in a global period. If a patient comes in on day 88 of a 90-day global period for a routine surgical follow-up, and the provider accidentally bills a Level 3 visit, it constitutes a false claim. Elite billing systems flag patients in global periods automatically to prevent accidental fraudulent billing.
5. Deep Dive: Orthopedic & Pain Management Billing
Orthopedic and Pain Management billing is arguably the most complex discipline due to extreme anatomical specificity and laterality requirements.
- Laterality is Mandatory: Submitting a claim for a knee injection without the RT (Right) or LT (Left) modifier will result in an instant medical necessity denial.
- Spinal Coding Complexities: Spinal surgeries require precise coding of the exact interspaces and segments involved (e.g., L4-L5). Unbundling arthrodesis, laminectomy, and bone grafting codes incorrectly will trigger massive RAC audits.
- Fluoroscopic Guidance: In pain management, knowing when imaging guidance (fluoroscopy or ultrasound) is bundled into the primary injection code (like transforaminal epidurals) versus when it can be billed separately (like large joint injections) is a critical compliance necessity.
6. Deep Dive: Cardiology & Gastroenterology Billing
Cardiology
Cardiology billing is defined by complex rules surrounding cardiac catheterizations, stent placements, and pacemaker insertions. Coders must understand the hierarchy of the coronary arteries (Left Anterior Descending, Right Coronary Artery, Circumflex) to know which interventions can be billed together. Furthermore, diagnostic testing (EKGs, Echoes) frequently requires a Modifier 26 (Professional Component) if the test was performed in a hospital setting where the physician does not own the equipment.
Gastroenterology
GI billing is heavily scrutinized for the "screening vs. diagnostic" colonoscopy trap. If a patient comes in for a preventative screening colonoscopy (fully covered under the Affordable Care Act) and a polyp is found and removed, the procedure converts from a screening to a diagnostic/surgical procedure. The coder must append specific modifiers (like PT for Medicare or 33 for commercial payers) to ensure the patient is not unfairly hit with a massive deductible bill.
7. Case Study: Rescuing an Orthopedic Group’s Spine Revenue
The Unbundling Crisis
The Client: A specialized orthopedic spine surgery group in New York. They were executing highly complex, multi-level spinal fusions, but their denial rate was hovering at 22%. Commercial payers were aggressively rejecting their claims for "Bundled Services."
The Diagnosis: An Axon Claim surgical coding audit revealed that the group’s in-house biller (who only had a general coding certification) was improperly appending Modifier 59 to decompression codes (laminectomies) performed at the exact same interspace as the spinal fusions. According to strict NCCI edits, decompression is inherent to the fusion at the same level and cannot be billed separately. The payer was denying the entire claim due to the unbundling attempt.
The Axon Claim Intervention:
- We deployed an AAPC-certified Orthopedic Surgical Coder (CASCC) to overhaul their operative report templates.
- We initiated a CDI program, training the surgeons to explicitly document when a decompression was performed at a different spinal level than the fusion, which is the only time it can be billed separately.
- The Results: By ceasing the improper use of Modifier 59 and adhering strictly to spinal NCCI edits, the group’s clean claim rate for surgeries jumped to 98%. We recovered $210,000 in previously stalled surgical claims within 45 days.
8. Why Specialty Practices Must Outsource to Certified Experts
A certified professional coder (CPC) is qualified to bill for a family practice. They are not qualified to read a 4-page operative report for a transcatheter aortic valve replacement (TAVR).
To survive in specialty medicine, practices must employ coders who hold specialty-specific certifications from the AAPC (e.g., CCC for Cardiology, CGIC for Gastroenterology, CASCC for Ambulatory Surgery). Because it is prohibitively expensive for an independent clinic to hire and retain multiple specialty-certified coders, top-tier practices outsource their RCM to premium partners like Axon Claim. By doing so, they gain instant access to a dedicated SWAT team of specialty coders who live and breathe complex surgical edits.
9. Conclusion
Specialty medical billing is an unforgiving financial environment. Insurance payers rely on the fact that surgical coding is overwhelmingly complex; they deploy automated NCCI engines to deny claims at the slightest hint of unbundling or modifier abuse, knowing that many practices lack the specialized expertise to successfully appeal.
By mastering the Global Surgical Period, applying Modifiers 25 and 59 with defensive precision, and partnering with highly certified surgical coders, specialty practices can break through the bureaucratic red tape. Do not let insurance payers discount your surgical expertise. Code accurately, appeal aggressively, and protect your high-dollar revenue.
Axon Claim LLC – Specialty Surgical Coders
We are a premier Revenue Cycle Management partner dedicated to helping specialty healthcare providers across NY, NJ, and the US maximize their revenue. Our AAPC-certified surgical coders master NCCI edits and complex global periods to protect your cash flow.
Are You Losing High-Dollar Surgical Revenue?
Unbundling errors and modifier mistakes trigger massive payer denials. Let our AAPC-certified specialty coders audit your surgical operative reports for free.
Request a Coding AuditMaximize Your Surgical Reimbursement